Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Sohit Karol
Kyung Koh
Hyun Joon Kwon
Yang Sun Park
Young Ha Kwon
Jae Kun Shim
http://dx.doi.org/10.5103/KJSB.2016.26.1.93 Epub 2016 April 20
Abstract
Objective: The purpose of this study was to investigate the effect of transcutaneous electrical nerve stimulation (TENS) treatment on maximum voluntary force (MVF) production.
Methods: Ten healthy, young subjects (5 males and 5 females) participated in the study. MVF was recorded after a fifteen minute session of TENS stimulation under two conditions: low frequency (4 Hz) at maximum tolerable level and high frequency (110 Hz) at maximum tolerable level. TENS was provided simultaneously via self-adhesive electrodes placed on the finger pads of the index, middle, ring and little fingers. MVF was also recorded in a baseline condition with no TENS treatment. Data were collected in three different sessions on three consecutive days at the sametime of the day.
Results: Results from the study show that on an average, MVF increasesby 25% for the index, middle and little fingers for TENS treatment with 4 Hz frequency as compared to the baseline condition. However, the 110 Hz condition did not result in a significantly different MVF than the baseline condition during individual finger pressing tasks. In addition, while producing MVF with all the four finger stogether, MVF was 30% higher for the 4 Hz conditionin comparison to the baseline condition, and 15% higher for the 110 Hz condition in comparison to the baseline condition respectively.
Conclusion: The results suggest that stimulation ofafferent fibers onthe glabrous skinwith TENS could have a net facilitatory effect on the maximum motoroutput.
Keywords
Finger Maximum finger force Nerve simulation Treatment
Cutaneous feedback is one of the primary sensory modalities for successful completion of day-to-day dex- terous manipulation tasks (Augurelle, Smith, Lejeune, & Thonnard, 2003; Johnson, 2001) and loss of cutaneous feedback from the fingers has been reported to produce lower magnitudes of maximum voluntary force (MVF) pro- duction (Augurelle et al., 2003; Shim et al., 2012). Lower MVF by the fingers is known to be a predictor of poor general health conditions (Sayer et al., 2006).
Although it is well established that loss of cutaneous feedback results in a decrease in maximal force production (Augurelle et al., 2003; Shim et al., 2012), if the maximum motor output could be enhanced by increasing the cuta- neous feedback from the fingers is not yet known. In recent years, transcutaneous electrical nerve stimulation (TENS) has emerged as an important treatment to enhance the cutaneous sensation in patients with sensory deficits (Celnik, Hummel, Harris-Love, Wolk, & Cohen, 2007; Dickstein & Kafri, 2008). Although the exact neurophysiological mechanism of this phenomenon is not yet known, it has been suggested that TENS could enhance the somato- sensory input by selectively stimulating certain afferent fibers, which in turn could modulate the motor output (Akyuz, Guven, Ozaras, & Kayhan, 1995; Urasaki, Wada, Yasukouchi, & Yokota, 1998). Further, different parameters of TENS are known to have a varied effect on the neuro- muscular system, and frequency of TENS stimulation has been shown to be one of the most important parameters (Chesterton, Foster, Wright, Baxter, & Barlas, 2003; Walsh, Foster, Baxter, & Allen, 1995).
The purpose of this study is to investigate the effect of low frequency (4 Hz) TENS as well as relatively high fre- quency (110 Hz) TENS on MVF production during multi-digit pressing. It has been hypothesized that TENS treat- ment would facilitate the motor output by enhancing the cutaneous feedback during multi-digit pressing, thus re- sulting in greater MVF.
1. Subjects
Ten healthy young volunteers (5 males and 5 females, age: 21.0±2.3 years) participated in the study. These in- dividuals were screened for any history of neurological disorders and were right handed according to the criteria of the Edinburgh handedness test. Participants were also administered a questionnaire to check their eligibility for TENS treatment and screen for any potential risks due to TENS. The experimental protocol was approved by the Institutional Review Board (IRB) of University of Maryland.
2. Experimental setup
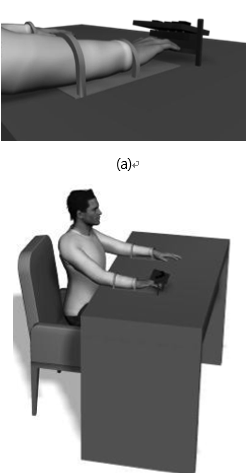
Customized equipment consisting of four one-dimensional force sensors was used to measure the maximal finger forces (Models 208 M182 and 484B, Piezotronics Inc., Depew, NY, USA). C-shaped aluminum thimbles were fixed at the bottom of each sensor in order to rest the distal ends of the fingers while pressing. The sensors were attached to an aluminum frame with four slits, allowing for the adjustment of sensor position based on the subject's finger size. The subject's hand were bent slightly at the metacarpophalangeal joint (MCP), proximal interphalangeal joint (PIP) and distal interphalangeal joint (DIP) in order to make a dome shape, when the fingers rested on the testing equipment (Figure 1).
The frame was tilted 25 degrees with respect to the anterior-posterior axis and attached to a vertical aluminum panel. This panel had a slit allowing for two degrees of freedom: vertical translation and rotation around the z-axis. During the experiment subjects pressed down on the C- shaped thimbles. The forces produced by the fingers were transmitted to the sensors. The signals from the sensors were set at 1,000 Hz with a 16-bit A/D board (PCI6034E, National Instruments Corp., Austin, TX, USA) and were recorded by a software program created in LABVIEW (Lab- VIEW 7.1, National Instruments Corp., Austin, TX, USA). Force production data was transferred to a computer adjacent to the testing room. MatLAB (MatLAB7, MathWorks, Inc, Natick, MA, USA) programs were written for data pro- cessing and analysis.
3. Procedure
Five different finger combinations (four single-finger tasks and one four-finger task) for the MVF task were presented to the subjects. The subject performed the task once per each condition. The five conditions were pre- sented to the subjects in a randomized order, with an interval of 3 min between consecutive pressing conditions. Once the subjects had comfortably positioned their fingers on their sensors, the investigators started the data collec- tion program, which generated a "get ready" sound. This was followed by a "ding" sound after 2s. Subjects were instructed to "press as hard as possible with the task finger and relax the fingers once they feel they cannot press any harder". After 7s, another audio cue in the form of a "ding" sound was presented to indicate the end of the trial. No visual feedback was provided to the subjects.
This process was repeated for three different experi- mental conditions; 1) baseline, 2) 4 Hz. TENS treatment, and 3) 110 Hz TENS treatment. TENS was delivered via a portable unit (Elpha 3000 II, Danmeter A/S, biphasic, pulse width 200 μs) with circular, self-adhesive electrodes on the distal phalanges of index, middle, ring and little finger for fifteen minutes before pressing the sensors. During the MVF task with individual finger, TENS was provided to the corresponding finger and during the task with all fingers, TENS was delivered to all fingers. The intensity was self-selected by participants and set to the maximum tolerable level. Data were collected on three different days at the same time of the day. The order of treatment conditions was randomly assigned to the subjects.
4. Data processing
Maximum voluntary force (MVF) was measured as the peak forces produced by task finger or fingers during single-finger tasks and a four-finger task.
The force deficit for each finger was calculated by taking the difference of the maximum force produced by an individual finger in a single finger task and subtracting it from the force produced by the same finger in the four finger task.
Due to various factors, when a single finger is instructed to produce a force, the other fingers also produce and unintentional force. This phenomenon has been called finger independence. The average values of FI across all the four fingers were calculated as shown below (Equation 2).
Where i ≠j, n=4, F_max^i is the maximal force pro- duced by the finger i and F^ij is the involuntary force produced by the non-task finger i during the i finger MVF task.
5. Statistics
One-way repeated measures ANOVAs were conducted to compare the MVF, FD and FI values between the three treatment conditions. The level of statistical significance was set at p=.05.
1. Maximum Voluntary Force (MVF)
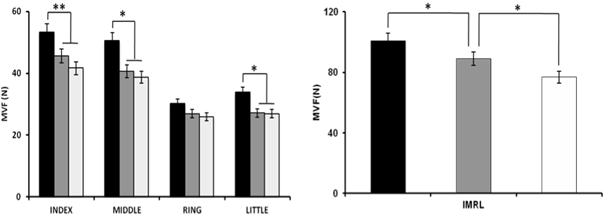
The MVF values for the single finger tasks increased significantly compared to the baseline condition for the index, middle and little fingers after 4 Hz TENS treatment. Specifically, the MVF values increased 28% for the index finger (from 41.6±6.3 N to 53.2±7.2 N), 30% for the middle finger(from 39.9±5.2 N to 49.2±6.3 N) and 25% for the little finger (from 24.6±4.2 N to 31.3±3.9 N) (Figure 2a). No significant differences were observed for the ring finger task. Further, MVF values for the 110 Hz condition were similar to the baseline condition during the individual finger tasks. These results were supported by ANOVA (Index: F2,18 = 13.5; p<.01; Middle: F2,18 = 5.83; p<.05; Little: F2,18 = 6.05; p<.05). For the four finger pressing task, MVF values were 30% greater than the baseline for 4 Hz con- dition and 15% greater than the baseline for the 110 Hz condition. MVF increased from 77.0±9.2 N in the baseline condition to 89.0±11.6 N in the 110 Hz condition and 101.0±12.8 N in the 4 Hz condition (Figure 2b). The results were supported by ANOVA (F2,18 = 8.94; p<.01).
2. Force Deficit (FD)
No significant differences in FD were found with TENS treatment.
3. Finger Independence (FI)
No significant differences in FI were found with TENS treatment.
Maximum voluntary force (MVF) production by the digits is vital to perform everyday activities and its importance is well documented in the literature (Sayer et al., 2006; Slobounov, Johnston, Chiang, & Ray, 2002; Yue & Cole, 1992). Although TENS has typically been used as a modality of somatosensory stimulation to mitigate pain, the neuro- physiological mechanisms of TENS are thought to excite the cortical motoneurons and affect motor output as well (Akyuz et al., 1995). While low intensity, high frequency somatosensory stimulation is known to significantly affect the motor output in humans, animal studies have sug- gested low frequencies could achieve similar results (Akyuz et al., 1995; Luft, Manto, & Ben Taib, 2005; Tinazzi et al., 2005; Walsh et al., 1995). Therefore, this study was unde- taken to investigate the effect of TENS treatment with low and high frequencies on MVF during multi-digit pressing. Participants described that the 4 Hz condition gave them a "piercing" sensation, while the 110 Hz condition gave them a "tingling" sensation.
Consistent with our hypothesis, MVF increased signifi- cantly with TENS treatment in comparison to the baseline condition. Specifically, 4 Hz condition produced greater MVF as compared to the baseline condition and the 110 Hz condition for index, middle and little fingers. No signifi- cant differences were observed for MVF in the ring finger among the three experimental conditions, although the data exhibited a similar trend of higher MVF values of index, middle and little fingers with 4 Hz frequency. The ring finger is most difficult to control due to the fact that flexors and extensors are shared with other fingers and cortical neurons responded to movement of the ring fingers coupled with those of other fingers. Thus, it may lead to no changes in MVF in the ring finger. However, it needs to have further investigation for better understanding of TENS effect on the ring finger control.
However, no changes in MVF were observed in individual finger tasks after 110 Hz TENS treatment. In addition, 4 Hz condition produced greater MVF for all the four fingers pressing together, followed by 110 Hz and baseline con- dition respectively. 110 Hz TENS treatment also produced greater MVF values than the baseline conditions for all the four fingers pressing together.
The experimental setup for this study afforded to stimu- late the finger pads and had a minimal effect on the intrinsic or extrinsic muscles of the hand directly. Thus, changes in motor output due to neuromuscular stimulation, as observed in some previous studies (Dickstein & Kafri, 2008), could therefore be ruled out in this study and the findings could be attributed to changes in somatosensory inputs alone. Previous studies providing visual or auditory feedback during maximum force production have shown a significant increase in force magnitude with the presence of appropriate sensory feedback (Kellis & Baltzopoulos, 1996; Sahaly, Vandewalle, Driss, & Monod, 2001). These studies suggest that under normal conditions, there is about 25~30% motor reserve which is not utilized typically and can be tapped into by using different methods like providing verbal motivation, visual or auditory feedback of force production.
Low frequency somatosensory stimulation of peripheral nerves has been known to increase the motor evoked potential as well as corticomotor excitability in previous studies (Mima et al., 2004; Nardone & Schieppati, 1989). Results from this study suggest that the increase in motor output could depend on TENS frequency as well as the digits involved in the task. Increase in MVF after short term TENS treatment (i.e., 30-minute TENS per a day) is consistent with results from such studies. The significant increase in MVF with short term TENS is encouraging and should be followed up with more elaborate studies to establish the most optimal combination of TENS para- meters to obtain maximum motor output.
Cutaneous feedback is known to be one of the major sensory modalities affecting the MVF production by the fingers of the hand (Collins, Knight, & Prochazka, 1999; Shim et al., 2012). Although the exact neurophysiological mechanism of changes in cutaneous sensation with TENS is not yet known, it has been shown that TENS treatment could temporarily increase the cutaneous sensitivity (Urasaki et al., 1998). TENS is thought to gate the somatosensory input at the peripheral level, through large afferent fibers and centrally through the cuneate nucleus (Luft et al., 2005; Nardone & Schieppati, 1989). There are four classes of low-threshold mechanoreceptors in human glabrous skin innervated by four classes of peripheral afferent nerve fibers. The neurons in the primary motor cortex have receptive fields in the periphery that receive inputs from the primary somatosensory cortex (Johansson, 1998). It is possible that low frequency TENS increased the cutaneous feedback, therefore changing the inputs to the primary somato- sensory cortex, which in turn facilitate the inputs to the motor cortex, thus resulting in an increased motor output. These results are consistent with our recent study where MVF values decreased with the removal of cutaneous feed- back (Shim et al., 2012).
It is noteworthy that in most of the previous studies, high frequency TENS has been applied at sub threshold or threshold levels of detection (Mima et al., 2004). In contrast, this study used high intensity TENS for both the 4 Hz as well as the 110 Hz condition. High frequency TENS at sub-threshold intensity has been shown to produce sig- nificant improvements in hand motor performance (Mima et al., 2004). No changes in MVF for individual fingers observed in this study with 110 Hz frequency suggest that the neurophysiological mechanisms involved in motor facili- tation could change depending on the combination of frequency and intensity of TENS and could be task depen- dent. It has been speculated that sub-threshold TENS enhances motor performance through the phenomenon called stochastic resonance (Manjarrez et al., 2002; Moss, Ward, & Sannita, 2004; Richardson, Imhoff, Grigg, & Collins, 1998). However, at higher intensities of TENS, like those employed in the current study suggest a mechanism of motor facilitation that is completely different from sto- chastic resonance.
In conclusion, this study provides an important tech- nique to enhance the MVF production capacity by em- ploying low frequency, high intensity TENS.
References
1. Akyuz, G., Guven, Z., Ozaras, N. & Kayhan, O. (1995). The effect of conventional transcutaneous electrical nerve stimulation on somatosensory evoked potentials. Elec- troencephalography and Clinical Neurophysiology, 35(6), 371-376.
Crossref
Google Scholar
2. Augurelle, A. S., Smith, A. M., Lejeune, T. & Thonnard, J. L. (2003). Importance of cutaneous feedback in main- taining a secure grip during manipulation of hand-held objects. Journal of Neurophysiol, 89(2), 665-671.
Crossref
Google Scholar
PubMed
3. Celnik, P., Hummel, F., Harris-Love, M., Wolk, R. & Cohen, L. G. (2007). Somatosensory stimulation enhances the effects of training functional hand tasks in patients with chronic stroke. Archives of Physical Medicine and Rehabilitation, 88(11), 1369-1376.
Crossref
Google Scholar
4. Chesterton, L. S., Foster, N. E., Wright, C. C., Baxter, G. D. & Barlas, P. (2003). Effects of TENS frequency, intensity and stimulation site parameter manipulation on pres- sure pain thresholds in healthy human subjects. Pain, 106(1-2), 73-80.
Crossref
Google Scholar
PubMed
5. Collins, D. F., Knight, B. & Prochazka, A. (1999). Contact-evoked changes in EMG activity during human grasp. Journal of Neurophysiol, 81(5), 2215-2225.
Crossref
Google Scholar
PubMed
6. Dickstein, R. & Kafri, M. (2008). Effects of antecedent TENS on EMG activity of the finger flexor muscles and on grip force. Somatosensory & Motor Research, 25(2), 139-146.
Crossref
Google Scholar
PubMed
7. Johansson, R. S. (1998). Sensory input and control of grip. Novartis Foundation Symposia, 218, 45-59.
Crossref
Google Scholar
PubMed
8. Johnson, K. O. (2001). The roles and functions of cutaneous mechanoreceptors. Current Opinion in Neurobiology, 11(4), 455-461.
Crossref
Google Scholar
PubMed
9. Kellis, E. & Baltzopoulos, V. (1996). Resistive eccentric exercise: effects of visual feedback on maximum moment of knee extensors and flexors. Journal of Orthopaedic and Sports Physical Therapy, 23(2), 120-124.
Crossref
Google Scholar
PubMed
10. Luft, A. R., Manto, M. U. & Ben Taib, N.O. (2005). Modu-ation of motor cortex excitability by sustained peri-heral stimulation: The interaction between the motor cortex and the cerebellum. Cerebellum, 4(2), 90-96.
Crossref
Google Scholar
PubMed
11. Manjarrez, E., Rojas-Piloni, J. G., Mendez,I., Martinez, L., Velez, D., Vazquez, D. & Flores, A. (2002). Internal stochastic resonance in the coherence between spinal and cortical neuronal ensembles in the cat. Neuroscience Letters, 326(2), 93-96.
Crossref
Google Scholar
12. Mima, T., Oga, T., Rothwell, J., Satow, T., Yamamoto, J., Toma, K. & Nagamine, T. (2004). Short-term high-frequency transcutaneous electrical nerve stimulation decreases human motor cortex excitability. Neuroscience Letters, 355(1-2), 85-88.
Crossref
Google Scholar
13. Moss, F., Ward, L. M. & Sannita, W. G. (2004). Stochastic resonance and sensory information processing: a tutorial and review of application. Clinical Neurophysi- ology, 115(2), 267-281.
Crossref
Google Scholar
PubMed
14. Nardone, A. & Schieppati, M. (1989). Influences of trans- cutaneous electrical stimulation of cutaneous and mixed nerves on subcortical and cortical somato- sensory evoked potentials. Electroencephalography and Clinical Neurophysiology, 74(1), 24-35.
Crossref
Google Scholar
15. Richardson, K. A., Imhoff, T. T., Grigg, P. & Collins, J. J. (1998). Using electrical noise to enhance the ability of humans to detect subthreshold mechanical cutaneous stimuli. Chaos: An Interdisciplinary Journal of Nonlinear Science, 8(3), 599-603.
Crossref
Google Scholar
16. Sahaly, R., Vandewalle, H., Driss, T. & Monod, H. (2001). Maximal voluntary force and rate of force develop- ment in humans—importance of instruction. European Journal of Applied Physiology, 85(3-4), 345-350.
Crossref
Google Scholar
PubMed
17. Sayer, A. A., Syddall, H. E., Martin, H. J., Dennison, E. M., Roberts, H. C. & Cooper, C. (2006). Is grip strength associated with health-related quality of life? - Findings from the Hertfordshire Cohort Study. Age and Ageing, 35(4), 409-415.
Crossref
Google Scholar
PubMed
18. Shim, J. K., Karol, S., Kim, Y. S., Seo, N. J., Kim, Y. H., Kim, Y. & Yoon, B. C. (2012). Tactile feedback plays acritical role in maximum finger force production. Journal of Biomechanics, 45(3), 415-420.
Crossref
Google Scholar
PubMed
19. Slobounov, S., Johnston, J., Chiang, H. & Ray, W. J. (2002). Motor-related cortical potentials accompanying en- slaving effect in single versus combination of fingers force production tasks. Clinical Neurophysiology, 113(9), 1444-1453.
Crossref
Google Scholar
20. Tinazzi, M., Zarattini, S., Valeriani, M.,Romito, S., Farina, S., Moretto, G. & Abbruzzese, G. (2005). Long-lasting modulation of human motor cortex following pro- longed transcutaneous electrical nerve stimulation (TENS) of forearm muscles: evidence of reciprocal in- hibitionand facilitation. Experimental Brain Research, 161(4), 457-464.
Crossref
Google Scholar
21. Urasaki, E., Wada, S., Yasukouchi, H. & Yokota, A. (1998). Effect of transcutaneous electrical nerve stimulation (TENS) on central nervous system amplification of somatosensory input. Journal of Neurology, 245(3), 143-148.
Crossref
Google Scholar
22. Walsh, D. M., Foster, N. E., Baxter, G. D. & Allen, J. M. (1995). Transcutaneous electrical nerve stimulation. Relevance of stimulation parameters to neurophysiological and hypoalgesic effects. American Journal of Physical Medi- cine & Rehabilitation, 74(3), 199-206.
Crossref
Google Scholar
23. Yue, G. & Cole, K. J. (1992). Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractions. Journal of Neurophysiology, 67(5), 1114-1123.
Crossref
Google Scholar
PubMed
