Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Sojung Lee
Dawun Jeong
Dong-Eun Kim
Kyungock Yi
http://dx.doi.org/10.5103/KJSB.2017.27.3.229 Epub 2017 October 15
Abstract
Objective: The purpose of this study was to identify the effects of taping therapy and inner arch support on pes planus lower extremity alignment and gait.
Method: The study was conducted on 13 women in their 20s who had pes planus and no gait problems. Independent variables were the condition of wearing basic socks (S1) and the condition of wearing socks with taping therapy and inner arch support (S2). The dependent variables were resting calcaneal stance position (RCSP), plantar pressure distribution during gait, and underlying and medial longitudinal arch angle measured using radiography. Statistical analysis was performed using the Wilcoxon test with SPSS 23.0 for comparison of S1 and S2.
Results: In the RCSP measurement, the angle range of S2 changed to normal. Meary’s angle appeared to be less than the angle of S1, indicating alleviation of the degree of pes planus. The calcaneal pitch angle increased at S2 from that at S1. The plantar pressure distribution was divided into four areas (toe, forefoot, midfoot, and hindfoot). At S2, the maximum pressure increased in the toe and midfoot. The maximum force increased significantly in the toe and midfoot but decreased significantly in the forefoot and hindfoot. In addition, the contact area increased overall especially at the midfoot and hindfoot. Contact time decreased in the toe and forefoot, but increased in the midfoot and hindfoot.
Conclusion: Taping therapy and inner arch support showed structural improvement of the pes planus. In addition, the force and pressure applied to the foot during walking are distributed evenly in the area of the sole, thus positively affecting walking.
Keywords
Plantar foot Inner arch support Foot pressure
The feet not only support the human body when standing but also absorb and distribute the impact from weight during walking (Seoul National University Hospital, 2003). For this main role, the foot has a unique structure called the arch (Kang, 2012). The foot has four arches, including the medial and lateral arches, and the anterior transverse arches of the forefoot and midfoot. Loss of the foot arch is associated with loss of dorsiflexion and plantarflexion abilities of the ankle joint, which is important for shock absorption, and may lead to various disabilities (SNUH, 2003). The pes planus, with the medial foot arch lowered and the entire sole of the foot touching the floor, leads to inadequate gait due to decreased impact absorption of the foot and excessive pro- nation movement (Song, 2008) and may accompany not only spasticity and heel pain, but also the hallux valgus or plantar fasciitis (Ministry of Health and Welfare, 2016).
The results of the footprint analysis performed for women in their 20~50s by the Korea Foot Health Association indicated that 84.8% of the women showed arch deformities such as pes planus and pes cavus, and 54.5% had hallux valgus (Lee, 2006). Thus, a taping technique and foot support to relieve or treat the symptoms of arch-foot deformity are needed (Lee et al., 2006). Taping is used for the prevention of injuries and any recurrence on the injured areas, and has a positive effect on the range of motion of the joints, joint fixation and muscle compression, and joint strength and muscle fatigue (Kang, Kim, & Lee, 2010; Park, 2008). Moreover, taping therapy applied to the ankle area reduces inversion and eversion of the ankle and affects the range of motion (Choi, 2007). In particular, foot taping therapy improves exercise performance by alleviating the pain during walking and induces a positive structural change to the foot arch (Jang et al., 2008; Lee, Kim, & Choi, 2009).
The force loaded on the feet daily is approximately 700 tons, while the feet takes more than 3,000,000 steps per year for a 70-kg person walking 10,000 steps per day (Lee, 2001). According to previous studies on foot supports for alleviating illness and symptoms caused by arch deformations, customized insole and lower limb stabilization exercises had positive effects on foot fatigue and lower body alignment/balance in adults with pes cavus (Ko, 2015). Lee (2006) also reported that foot support and lumbar stabilization exercises caused changes in the angles of the foot, pelvis, and lumbar. Park (2008) showed that the use of a foot aid changed the mean value of the ankle angle to nearly normal at the sagittal plane. Park showed that the foot aid had an independent positive effect on the stabilization of the foot. As such, research studies are actively being conducted on the immediate effect of using foot orthosis and on the functional shoe that supports the medial arch by using the structure of the insole. However, the limitation was that the effects of the foot orthosis and insole were not obtained when the shoes were taken off, which makes a substitute necessary so that the effect of wearing arch support can be achieved even when not wearing shoes. Therefore, the purpose of this study was to place an inner arch support inside the sock and to investigate how the sock integrated using the inner arch-fixing taping method affects the lower leg alignment and pes planus during walking.
1. Participants
In this study, 13 women who were flat-footed in their 20s and had no injuries to their lower extremities or any other injuries were selected. The measured foot of each subject was controlled to be the right foot, and the experiment was conducted for 2 days from August 23, 2016, to August 24, 2016. The mean age of the subjects was 24.77 ± 3.00 years. The mean height and body weights were 161.72 ± 4.52 cm and 54.08 ± 3.95 kg, respectively (Table 1).
|
|
Age (yrs) |
Height (cm) |
Weight (kg) |
|
Mean ± SD |
24.77 ± 3.00 |
161.72 ± 4.52 |
54.08 ± 3.95 |
|
N |
13 |
13 |
13 |
2. Variables
The independent variables in the experiment were (Table 2) wearing a sock without any treatment (S1), and wearing a sock with an inner arch support and taping therapy (S2). Dependent variables were resting calcaneal stance position (RCSP), maximum pressure on each foot area, contact area, contact time, lower extremity alignment angle, calcaneal pitch angle, and Meary's angle (Table 3).
|
Variable |
Sock structure |
Features |
|
S1 |
|
Socks |
|
S2 |
|
Taping therapy on socks with inner arch support |
|
Resting
Calcaneal Stance Position (RCSP) |
Foot pressure |
Radiography |
|
|
|
|
3. Measurements
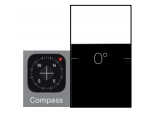
The test socks were made as shown in (Table 4). The inner arch support (Implus Footcare LLC, China) was placed inside the sock, and taping therapy was applied to support for ankle fixation and the inner arch as shown in (Table 5). The final design of the socks is shown in (Figure 1). (Table 6) shows the measurement tools used in this study. Compass (Apple Inc., USA), a smartphone application for angle measurement, was used to measure the RCSP of the subjects. The smart application for angle measurement is quite accurate to measure the angle of the knee flexion or body angles, and Compass is also useful as an alternative to the portable goniometer and is as common as the goniometer smartphone application (Jenny, 2013; Milani et al., 2014). The smartphone was placed on a flat surface, and the angle between the line bisecting the calcaneus and the line vertical to the ground was measured to measure the level of the flat feet (pes planus). Radiographic images were taken from the coronal plane to view the lower extremity alignment and from the sagittal plane to view the calcaneal pitch angle of the foot and Meary's angle between the talus and the first metatarsal. To analyze plantar pressure, foot pressure data were collected at 50-60 Hz/s by using the Novel company’s emed platform and during walking in accordance with the stride of each subject, while the walking speed was controlled using a metronome (Panoramic Software Inc., USA).
|
|
Composition |
Features |
|
Socks |
|
Knee socks (Sapin, Korea) Materials: cotton and Length: 32 cm |
|
Inner |
|
Air+ Perfect Comfort Length: 28 cm, Height: 12.7 cm |
|
Kinesio |
|
Original Kinesio tape Materials: cotton 96% Length: 5 m, Width: 5 cm |
|
|
Taping therapy |
Process |
|
Ankle support |
|
Taping from the calf muscle to the inner
calf muscle through |
|
Ankle arthrodesis |
|
The tape was fixed at the center of the
medial arch and stuck in the direction of the back of the ankle through the
foot. Over the Achilles tendon of the heel, across
the back of the foot across the outer arch, the tape is overlaid in the
middle of the foot. |
|
Arch support |
|
Taping in the medial phalanx to support the
ankle medial |

|
Compass |
Emed |
Metronome |
|
|
|
|
4. Data processing
1) Resting calcaneal stance position
The RCSP is the angle between the bisector of the calcaneus (the heel bone) and the floor in an upright position. The measurement method is shown in (Figure 2). First, the subject was placed on a flat surface, and the center line of the calcaneus was marked. Then, the angle between the center line marked with the line on the floor and the vertical line on the ground was measured (Kang, 2012). The calcaneus angle was measured using a smartphone angle application (Compass, Apple Inc.). If the value was negative and the bisector of the calcaneus tilted inward, the subject had pes cavus; if the value was positive while the bisector tilts to the outside, the subject had pes planus (Yi, Kim, & Kim, 2012). The RCSP measurement showed that the method of checking for pes planus had an error range of 1° or less when compared with the radio- graphic measurement value, thus proving its reliability as a method of classifying the foot type (Hayes, 1992; Menz, 1995). Feet were classified as normal if the measured value was -2° or more, or 2° or less, narrow if the angle was 3° or more, and flat if the value was -3° or less (Song et al., 1996; Valmassy, 1996; Kim, 2013). To reduce the error between researchers, the same researcher measured the RCSP of the subject's right foot repeatedly three times for either the wearing of the basic sock (S1) or the test sock (S2).

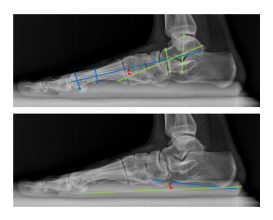
2) Radiography
Radiographic images were analyzed to confirm the changes of the lower leg alignment, the calcaneal pitch angle, and Meary's angle (angle between the talus and the first metatarsal) from wearing the basic sock (S1) to wearing the test sock (S2). The subject was asked to wear the basic sock (S1) and then the test sock (S2), in the respective order, and images were taken in the coronal plane for the lower body and in the sagittal plane for the foot.
(Tables 7 and 8) show the measurement line and angle measurement method for the pelvis, femur, lower leg, angle of the medial arch of foot, and first metatarsal. With reference to the previous study (Jeong, 2016), radiographic images were printed and the angle of each line was measured by marking the reference line. For the pelvis, an extension line was drawn between the iliac crest in a frontal posture while supporting the weight, and the tilted value in a neutral posture-maintaining level was used for analysis. The reference points for the femur and lower leg were at the midpoint of the femur and patella, and the midpoint of the tibia abutting the talus, respectively. The medial arch of the foot was marked by the baseline of the lower half of the calcaneus, the bisector of the talus, and the bisector of the first metatarsal. To reduce the error, one researcher marked the center point of each joint and the baseline, and repeated the measurement three times; the average was used for analysis.
|
|
Lower
leg |
Foot |
|
Guide
line |
|
|
|
|
Lower
leg |
Foot |
|
Guide
line |
|
|
|
Variable |
Measurement
method |
|
Pelvic
alignment |
Posterior
iliac crest in frontal weight-bearing posture angle of horizon |
|
Femoral |
Femur-to
-medial point of the patella: |
|
The
lower leg alignment |
Center
point of the patella: The angle |
|
Calcaneal |
The
angle between the bottom of the |
|
Meary's angle |
Lateral
talo-first metatarsal angle |
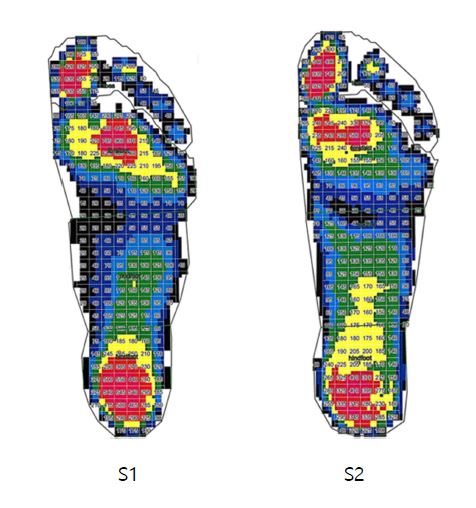
3) Plantar pressure analysis
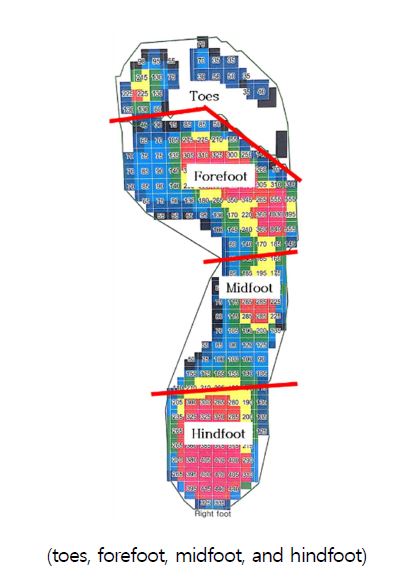
For the analysis of plantar pressure during walking, the maximum pressure, maximum force, and area and duration of contact with the ground were measured with the wearing of the basic sock (S1) and test sock (S2). To evaluate the effect of taping therapy and inner arch support on foot movements, the foot area was divided into four parts, namely toes, forefoot, midfoot, and hindfoot (Figure 3).
In the experiment, the subjects were asked to wear the basic sock (S1) and then the test sock (S2) in this sequence and perform the 4-step walking in accordance to the normal stride of each subject. At the last support period of the walking, the right foot was naturally passed through the emed platform (Novel, German). The walking speed was set at 82 bpm of 1/4 beat by using a metronome (Panoramic Software Inc., USA) to control the average speed of adult walking at 1.3 m/sec. To reduce the error during the data collection, the subjects practiced enough to perform the natural gait following the beat of the metronome, and the experiment was repeated three times to obtain the average value for the analysis.
5. Statistical analysis
The data analysis was performed using SPSS 23.0. A nonparametric test was conducted, as the data were not normal because of the small number of samples (Jeong, 2002). The Wilcoxon test was used to compare and analyze the change in RCSP, leg alignment, foot angle, and plantar pressure distribution when switching from wearing the basic sock (S1) to wearing the test sock (S2).
1. Analysis of RCSP on taping and inner arch support
The measured values of the standing angle (RCSP) measured when stable were -4.08° ± 2.57° with the basic sock and 1.69° ± 3.01° with the test sock, indicating the measured value changed to the normal range of -2° or more, or 2° or less with the test sock (Z = -2.936, p < .003; Table 9). A statistically significant difference was found between the two groups. Taping therapy and inner arch support provided structural improvement of the pes planus.
|
|
N |
Mean ± SD |
Z |
p-value |
|
S1 |
13 |
-4.08
± 2.57 |
-2.936 |
.003 |
|
S2 |
13 |
1.69 ± 3.01 |
2. Lower leg alignment analysis on taping and inner arch support
1) Pelvis alignment analysis
The measured pelvic angle was -.58° ± 1.68° when wearing the basic sock and -1.15° ± 1.77° when wearing the test sock, and no statistically significant difference was found (Z = -1.812, p > .070; Table 10).
|
|
N |
Mean ± SD |
Z |
p-value |
|
S1 |
13 |
-.580
± 1.68 |
-1.812 |
.070 |
|
S2 |
13 |
-1.15
± 1.77 |
2) Thigh alignment analysis
The thigh angle was measured as shown in (Figure 4). The thigh angle is the angle between the connecting line of the tibial tuberosity and the line extending across the patella from the thigh bone through the center of the patella. With the normal range of 87.5° ± 2.5°, an angle of less than 85° means that the thigh is in eversion and an angle greater than 90° means that the thigh is in inversion (Paley Orthopedic & Spine Institute, 2014). In this study, the mean changed from 88.62° ± 2.06° for the basic sock to 89.08° ± 2.14° for the test sock (Table 11). No statistically significant difference was found (Z = -1.303, p > .193), but the thigh angle increased when the test sock was worn, which suggests that the eversion of the thigh was somewhat alleviated.
|
|
N |
Mean ± SD |
Z |
p-value |
|
S1 |
13 |
88.62 ± 2.06 |
-1.303 |
.193 |
|
S2 |
13 |
89.08 ± 2.14 |
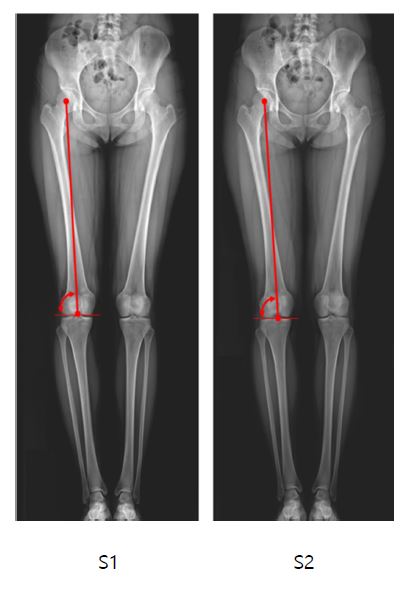
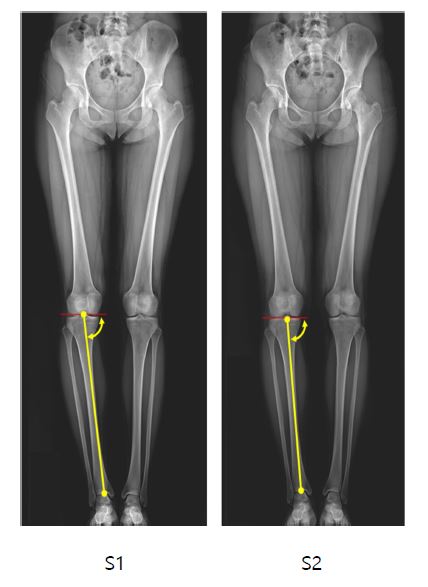
3) Lower leg alignment analysis
The angle of the lower leg is the angle between the line connecting the center of the patella to the center of the ankle and the line extending across the patella. A value greater than 90° means lower leg eversion, and an angle less than 90° means inversion (Paley Orthopedic & Spine Institute, 2014). The mean changed from 86.77° ± 2.13° for the basic sock to 87.08° ± 1.61° for the test sock (Figure 5, Table 12). No statistically significant difference was found (Z = -718, p > .473), but the inversion of the lower leg was somewhat alleviated when the test sock was worn.
|
|
N |
Mean ± SD |
Z |
p-value |
|
S1 |
13 |
86.77
± 2.13 |
-.718 |
.473 |
|
S2 |
13 |
87.08
± 1.61 |
4) Calcaneal pitch angle analysis
To determine if the taping and inner arch support have an immediate effect on the structural improvement of the flat feet, the calcaneal pitch angle and Meary's angle between the talus and the first metatarsal were analyzed (Table 13). On the basis of the calcaneal pitch angle with a normal range of 16.8° ± 5.6°, an angle less than 11.2° was classified as pes planus and an angle more than 22.4° was classified as pes cavus (University of Washington Department of Radiology, 2016). When the test sock was worn, the angle changed to 21.54° ± 3.82°, which was higher than that of the basic sock (19.62° ± 2.93°) within the normal range (Z = -2.858, p < .004).
Meary's angle was classified as pes planus when the baseline of the talus was angled below the first metatarsal baseline by more than 4° and as pes cavus when the baseline of the talus was angled above the first metatarsal baseline by 4° (University of Washington, Department of Radiology, 2016). The degree of pes planus or pes cavus can be evaluated depending on the angle. If it is less than 15°, 15~30°, or more than 30°, it is judged to be a weak pes planus/cavus, normal pes planus/cavus, or severe, respectively. The angle was 6.81° ± 2.80° when the test sock was worn, lower than that when wearing the basic sock (10.04° ± 4.70°), showing alleviation of the severity of the flat feet with a statistically significant difference (Z = -2.670, p < .008).
|
|
|
N |
Mean ± SD |
Z |
p-value |
|
Calcaneal pitch |
S1 |
13 |
19.62 ± 2.93 |
-2.858 |
.004 |
|
S2 |
13 |
21.54 ± 3.82 |
|||
|
Meary's
angle |
S1 |
13 |
10.04 ± 4.70 |
-2.670 |
.008 |
|
S2 |
13 |
6.81 ± 2.80 |
3. Gait analysis on taping and inner arch support
1) Peak pressure per sole area
The peak pressure per sole area is shown in (Figure 6) and (Table 14). The change was statistically significant in three areas, namely the toe, forefoot, and midfoot. The pressure significantly increased in the toes (Z = -3.180, p < .001) and midfoot (Z = -3.040, p < .002), while it significantly decreased in the forefoot (Z = -3.180, p < .001).
|
|
N |
Mean ± SD |
Z |
p-value |
|
|
Toes |
S1 |
13 |
7.19 ± 2.68 |
-3.180 |
.001 |
|
S2 |
13 |
10.16
± 3.70 |
|||
|
Forefoot |
S1 |
13 |
9.76 ± 4.71 |
-3.180 |
.001 |
|
S2 |
13 |
6.98 ± 2.80 |
|||
|
Midfoot |
S1 |
13 |
1.94 ± 0.55 |
-3.040 |
.002 |
|
S2 |
13 |
2.58 ± 0.32 |
|||
|
Hindfoot |
S1 |
13 |
6.20 ± 1.37 |
-.314 |
.754 |
|
S2 |
13 |
6.31 ± 1.72 |
|||
|
Total |
S1 |
13 |
10.91
± 4.35 |
-.734 |
.463 |
|
S2 |
13 |
11.52
± 4.04 |
|||
2) Maximum force per sole area
The change was statistically significant in all four areas (toe, forefoot, midfoot, and hindfoot). The maximum force significantly increased in the toes (Z = -3.180, p < .001) and midfoot (Z = -3.180, p < .001), while it significantly decreased in the forefoot (Z = -3.180, p < .001) and hindfoot (Z = -3.110, p < .002; Table 15).
|
|
N |
Mean ± SD |
Z |
p-value |
|
|
Toes |
S1 |
13 |
0.32 ± 0.11 |
-3.180 |
.001 |
|
S2 |
13 |
0.40 ± 0.11 |
|||
|
Forefoot |
S1 |
13 |
0.89 ± 0.11 |
-3.180 |
.001 |
|
S2 |
13 |
0.79 ± 0.11 |
|||
|
Midfoot |
S1 |
13 |
0.17 ± 0.06 |
-3.180 |
.001 |
|
S2 |
13 |
0.37 ± 0.05 |
|||
|
Hindfoot |
S1 |
13 |
0.74 ± 0.08 |
-3.110 |
.002 |
|
S2 |
13 |
0.67 ± 0.09 |
|||
|
Total |
S1 |
13 |
1.14 ± 0.06 |
-1.223 |
.221 |
|
S2 |
13 |
1.16 ± 0.06 |
|||
3) Contact area per sole area
Overall, the contact area increases for the test sock. Especially the contact area increased significantly in the midfoot (Z = -3.180, p < .001) and hindfoot (Z = -2.832, p < .002; Table 16).
|
|
N |
Mean ± SD |
Z |
p-value |
|
|
Toes |
S1 |
13 |
19.48 ± 3.25 |
-1.678 |
.093 |
|
S2 |
13 |
20.15 ± 2.42 |
|||
|
Forefoot |
S1 |
13 |
42.61 ± 3.91 |
-1.468 |
.150 |
|
S2 |
13 |
43.17 ± 3.10 |
|||
|
Midfoot |
S1 |
13 |
19.96 ± 5.13 |
-3.180 |
.001 |
|
S2 |
13 |
28.41 ± 2.25 |
|||
|
Hindfoot |
S1 |
13 |
27.71 ± 2.48 |
-2.832 |
.002 |
|
S2 |
13 |
29.17 ± 2.70 |
|||
|
Total |
S1 |
13 |
109.86 ± 11.49 |
-3.180 |
.000 |
|
S2 |
13 |
120.99
± 8.70 |
|||
4) Contact time per sole area
Changes were significant in all four areas (toe, forefoot, midfoot, and hindfoot). The toes (Z = -3.180, p < .001) and forefoot (Z = -3.113, p < .002) showed statistically significant decreases in contact time, while the midfoot (Z = -3.180, p < .001) and hindfoot (Z = -2.830, p < .005) showed significant increases (Table 17).
|
|
N |
Mean ± SD |
Z |
p-value |
|
|
Toes |
S1 |
13 |
78.52 ± 11.30 |
-3.180 |
.001 |
|
S2 |
13 |
70.57 ± 9.94 |
|||
|
Forefoot |
S1 |
13 |
86.29 ± 1.87 |
-3.113 |
.002 |
|
S2 |
13 |
84.00 ± 1.94 |
|||
|
Midfoot |
S1 |
13 |
59.49 ± 6.45 |
-3.180 |
.001 |
|
S2 |
13 |
66.35 ± 4.48 |
|||
|
Hindfoot |
S1 |
13 |
54.61 ± 4.55 |
-2.830 |
.005 |
|
S2 |
13 |
59.87 ± 5.10 |
|||
|
Total |
S1 |
13 |
100.00 ± 0.00 |
-.000 |
1.000 |
|
S2 |
13 |
100.00 ± 0.00 |
|||
1. The effect of taping and inner arch support on lower body alignment
The analysis of the angles of the pelvis, thigh, lower leg, first meta- tarsal angle, and medial arch of 13 women with pes planus showed no significant differences in the thigh and lower leg angles, but the angles of the right thigh and lower leg became closer to the normal range. This suggests that the degree of flatness of the sole of the study subjects was not so severe to begin with and did not show a significant change in the degree of asymmetry in the lower limb alignment. How- ever, taping therapy and inner arch support improved the alignment of the lower limbs, supporting the study that reported a positive effect of the insole on lower limb correction (Kim, 2011; Lee, 2006; Song, 2008).
In addition, the first metatarsal angle significantly decreased (Z = -2.670, p < .008) and the calcaneal pitch angle significantly increased (Z = -2.858, p <.004). This suggests that the medial arch was raised by wearing the test sock (S2) with taping and inner foot support, and that the structural problem of flat feet was improved by taping. Therefore, taping therapy and the use of an inner arch insole insertion sock have positive effects on not only the structure of the flat feet but also the alignment of the legs.
2. The effects of taping and inner arch support on gait
The gait analysis for the right foot showed that the peak pressure in the toe and midfoot significantly increased, while that in the forefoot significantly decreased. The maximum force was significantly increased in the toes and midfoot, but was significantly decreased in the fore- foot and hindfoot. This supports the study in which the maximum force of the midfoot increased while that in the hindfoot decreased when walking on a flat foot (Chang et al., 2010). The decreases in the peak pressure and maximum force in the forefoot and hindfoot distribute the pressure and impact applied to the foot from the ground, sup- porting the finding that the inner arch support has a positive effect on walking (Woo et al., 2015). Furthermore, the significant increase in the peak pressure and maximum force in the toe and the increase in contact area were caused by even use of the toes by using the inner arch support and the test sock with taping (S2), which according to a previous study (Yi, 2010), can correct toe deformations and strengthen muscles owing to the positive effect of the inner arch support and taping on walking.
The contact area was significantly increased in the midfoot and hind- foot, which supports the study that indicated that the midfoot ratio in the weight distribution increased during walking for pes planus (Chang et al., 2010). The contact time and peak pressure increased in the midfoot and hindfoot with the increase in contact area. This was due to the increase in the peak pressure and maximum force caused by the increases in contact area and contact time of the midfoot when the inner arch support was applied. The peak pressure and maximum force of the toe increased, the maximum force of the hindfoot decreased, and the contact areas of the toe and forefoot also increased, indicating that taping and the inner arch support evenly distribute force and pressure across the sole area, thus positively affecting walking. This study supports the previous study that reported that when an arch-like shape similar to a normal foot was applied to a flat foot, the pressure was distributed across the contact area just like a normal foot (Kim, 2006).
The purpose of this study was to investigate the immediate effects of taping and inner arch support on the lower body alignment and walking. The following conclusions were obtained: First, the angle of the inner arch increased within the normal range when the test sock (S2) designed with taping and inner arch support was worn, and the angle of the first metatarsal decreased within the normal range. In accordance with the criterion for determining the severity of pes planus, flat feet seemed to be alleviated by taping and inner arch support. Second, the peak pressure and maximum force of the toe increased and those of the hindfoot decreased, and the contact areas of the toe and forefoot also increased, which show that pressure is evenly distributed in the sole area, thereby positively affecting walking.
As the study was conducted with a small group of subjects with few of whom showing less than -2° of the RCSP, the effect was not significant. Nevertheless, the overall results showed that the taping and inner arch support immediately corrected the pes planus and had positive effects on gait. Subsequent studies on the classification of the hardness of the RCSP should be conducted.
References
1. Chang, J. S., Park, J. W. & Kim, C. S. (2010). The changes of plantar foot pressure by external loads during walking in flatfoot. Journal of the Korean Society of Physical Medicine, 5(4), 543-549.
Crossref
Google Scholar
2. Choi, J. Y. (2007). The Effects of Taping of Strength & postural Stablity on Ankle & Shoulder. Unpublished Master's Thesis. Graduate School of Education of Myoungji University.
Crossref
3. Hayes, K. W. (1992). The effect of awareness of measurement error on physical therapists' confidence in their decisions. Physical Therapy, 72, 515-525.
Crossref
Google Scholar
4. Jang, I. G., Kim, D. H., Yoo, J. O., Lee, S. H., Park, S. K., Choi, S. K., Hong, J. M., Kang, H. J., Sung, K. H., Lee, B. J., Kim, M. Y. & Kim, M. K. (2008). The effect of sports taping on the pain, exercise performance and structural changes of arch on X-ray. Korean Association of Certified Exercise Professionals, 2008(1), 801-804.
Crossref
5. Jeong, J. Y. (2016). The immediate effects of Jump Rope with or with- out visual Feedback on Foot Deformation and lower extremity Alignment Correction of a Flatfeet. Unpublished Master's Thesis. Graduate School of Ewha Womans University.
Crossref
6. Jeong, M. M. (2002). Types and application of nonparametric statistical methods. Korean Journal of Sport Science, 7, 47-58.
Crossref
7. Jenny, J. Y. (2013). Measurement of the knee flexion angle with a smartphone-application is precise and accurate. The Journal of Arthroplasty, 28, 784-787.
Crossref
Google Scholar
PubMed
8. Kang, H. S. (2012). The Validity of the Foot Deformity Measurement Method: Correlation between total-middle-body Width Ratio (CSI), trunk-to-hip Ratio Index (SAI), and Calcaneal Angle (RCSP). Unpub- lished Master's Thesis. Graduate School of Education of Ewha Womans University.
Crossref
9. Kang, J. H., Kim, S. H. & Lee, K. J. (2010). Taping of musculoskeletal Disorders learned with Pictures and Photographs. Seoul: Median Book.
Crossref
10. Kim, K. H. (2011). Biomechanical Analysis of Arch Support Devices on normal and low Arch. Unpublished Master's Thesis. Graduate School of Kyungsung University.
Crossref
11. Kim, N. H. (2013). The Effects of corrective Hip Joint Exercises and Foot Orthotics on RCSP, Ankle dorsi/plantar Flexion, pelvic Motion, core Muscle Strength, and Foot Pressure for middle School Students with Pes Planus. Unpublished Doctor's Dissertation. Graduate School of Ewha Womans University.
Crossref
Google Scholar
12. Ko, D. H. (2015). Effects of a customized Insole and Stabilization Exercise for lower extremity on Foot Fatigue, lower extremity Alignment, and Balance in pronated Adult Feet. Unpublished Doctor's Dissertation. Graduate School of Daegu University.
Crossref
13. Lee, C. W. (2006). Effects of Foot Orthoses and lumbar Stabilization exercise on spinal malaligment Patients with Flatfoot. Unpublished Master's Thesis. Graduate School of Sports Industry of Kookmin University.
Crossref
14. Lee, G. C., Kim, C. H., Kim, B. G., Kim, S. H., Kim, A. T., Yang, H. S., Yoon, Y. S., Lim, H. M., Jang, M. Y. & Jang, C. (2006). The effects of balanced performances on degree of dropped foot arch. Archives of Orthopedic and Sports Physical Therapy, 2, 45-52.
Crossref
15. Lee, J. K., Kim, Y. K. & Choi, J. H. (2009). Influence of orthopedic medical taping on gait of stance phase and pain. The Journal of Korean Society of Health Science, 6, 1-7.
Crossref
16. Lee, J. Y. (2001). Special relationship between diabetics and shoes. The Rubber Society of Korea, 2, 124-128.
Crossref
17. Lee, Y. L. (2006, October 10). Korean women 85%
Crossref
18. Menz, H. B. (1995). Clinical hindfoot measurement: a critical review of the literature Review Article. The Foot, 5, 57-64.
Crossref
Google Scholar
19. Milani, P., Coccetta, C. A., Rabini, A., Sciarra, T., Massazza, G. & Ferriero, G. (2014). Mobile smartphone applications for body position measurement in rehabilitation: a review of goniometric tools. Physical Medicine and Rehabilitation, 6, 1038-1043.
Crossref
Google Scholar
20. Ministry of Health and Welfare. (2016). National Health Information Portal. Retrieved January 14, 2017, from http://health.mw.go.kr/ HealthInfoArea/HealthInfo/View.do?idx=4360
Crossref
21. Paley Orthopedic & Spine Institute. (2014. n.d.). Blount's Disease. Retrieved Januaty 14. 2017. from http://www.paleyinstitute.org/ orthopedic-conditions/blounts-disease/blounts-disease
Crossref
22. Park, J. T. (2008). Research on the Effect of Kinesio Taping Method on muscular Strength and Fatigue. Unpublished Doctor's Dissertation. Graduate School of Myongji University.
Crossref
23. Park, K. Y. (2008). Study on changing the Angle of Ankle to the sagittal Plane with F. F. O before and after Wearing during the Walk. Un- published Master's Thesis. Graduate School of Alternative Medicine, Kyonggi University.
Crossref
24. Song, J., Hillstrom, H. J., Secord, D. & Levitt, J. (1996). Foot type biomechanics. comparison of planus and rectus foot types. Journal of the American Podiatric Medical Association, 86, 16-23.
Crossref
Google Scholar
25. Song, J. H. (2008). The kinematic comparative study about effects of foot orthotics. Korean Journal of Sport Science, 19, 11-21.
Crossref
26. Seoul National University Hospital. (2003). Body organs information. Retrieved March 5, 2017, from http://news.naver.com/main/ read.nhn?mode=LSD&mid=sec&sid1=103&oid=003&aid=0000200149
Crossref
27. University of Washington Department of Radiology. (2016. August 14). Pes Planus. retrieved August 10. 2017. from http://uwmsk.org/ footalignment/doku.php?id=pes_planus# other_measurements
Crossref
28. Valmassy, R. L. (1996). Clinical Biomechanics of the lower Extremities. St. Louis: Mosby
Crossref
29. Woo, J. H., Lee, J. S., Yang, J. O., Lee, B. J., Bae, K. H., Han, D. W., Park, S. M. & Bae, J. W. (2015). Analysis of plantar foot pressure according to lnsole types during treadmill gait. Korean Journal of Sport Biomechanics, 25(1), 113-122.
Crossref
Google Scholar
30. Yi, K. O. (2010). The effect of shoe type on plantar pressure distributions. Journal of Korean Association of Physical Education and Sport for Girls and Women, 24(4), 1-11.
Crossref
31. Yi, K. O., Kim, N. H. & Kim, Y. R. (2012). The differences in foot type according to major in left and right foot for female college students. Korean Society of Sport Biomechanics, 22, 229-236.
Crossref
Google Scholar