Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Ji-Seon Ryu
http://dx.doi.org/10.5103/KJSB.2017.27.1.45 Epub 2017 April 18
Abstract
Objective: The aim of this study was to investigate the periodicity of the lower extremity joint flexion/ extension angle to compare the local stability between young and elderly women during walking on a treadmill.
Method: Eighteen young women (mean age=21.2±1.6 y; mean mass=57.1±6.1 kg; mean height=1.61±0.04 m) and 18 elderly women (mean age=66.4±1.2 y; mean mass=55.4±8.3 kg; mean height=1.56±0.04 m) participated in this study. Approximate entropy (ApEn) was used to determine the periodicity in the lower limb joint angles.
Results: The ApEn values of the two groups were statistically greater in the surrogate data test than in the original time series data (p<.05). The periodicity of the hip and ankle flexion/extension angles decreased in the elderly women group compared with the young women group (p<.05). The periodicity of the lower extremity joint flexion/extension angle showed that the ankle joint increased dominatingly in both groups (p<.05); the hip joint decreased compared with the knee joint in the young women group; and the knee joint decreased compared with the hip joint in the elderly women group (p<.05).
Conclusion: These results suggest that the lower extremity joint flexion/extension angles of the young and elderly women during walking contained random noises as well as biological signals. In addition, the differences in the periodicity in the lower extremity joint between the young and elderly women may provide some insight in predicting potential falls and be used as a characteristic indicator for determining local stability in elderly women during walking.
Keywords
Approximate entropy Periodicity Local stability Walking Elderly women Falling Lower extremity joint
In 2015, the elderly population (≥65 years) accounted for about 13.2% of the total population in South Korea (Statics Korea, 2016). By 2020, the percentage is expected to exceed 15%, which is forecasted to reach up to 32% by 2040, with Korea becoming a super-aged society (Statics Korea, 2014). Health is one of the major concerns of the rapidly increasing elderly generation. However, the health of the elderly is being threatened by physical changes due to aging. A fall is considered one of the most dangerous factors that can harm the health of the elderly (Berry & Miller, 2008).
A fall is defined as a part of the body contacting the ground from unintentional loss of balance without any external impact while per- forming activities of daily living (Lord, Caplan, & Ward, 1993). Fall acci- dents in Korea are showing an increasing trend every year as well. In 2013, the number of fall accidents involving elderlies aged ≥65 years, as reported to the Korea Consumer Agency, was 294 cases, which in- creased by 35% each year to 402 cases in 2014 and 554 cases in 2015 (Health Chosun, 2017). Falls sometimes cause injuries, which can not only lead to high social costs for treating such injuries but also lower the quality of life (QoL) of the elderly. Falls account for 12% of all deaths among elderlies, representing the 6th most common cause of death (American Geriatrics Society, 2001; Curry & Hogstel, 2002). In this regard, falls among elderly individuals can only be viewed as a serious problem that degrades their QoL (Kauffman, 1999).
Tinetti et al. (1988) claimed that an individual's intrinsic factors, such as loss of balance and muscle function deterioration, play a bigger role in falls among elderlies than environmental factors. The lower extremity muscle functions of elderlies are highly correlated with their balance ability (Hausdorff, Mitchell, Goldberger, & Wei, 1997; O'Brien, Culbam, & Pickles, 1997; Song, Mun, Kang, & Choi, 2001; Wolfson, Judge, & Whipple, 1995); thus, it is no exaggeration to say that preventing falls among elderlies is dependent on their ability to maintain balance. Fall prevention is mostly based on an individual’s protective ability against balance disturbances (Johnell & Kanis, 2006). Therefore, it is necessary to analyze the stability maintained by balance when examining the predictive factors of falls among elderlies. Muscle mass decreases by 0.5~1% each year from the late 30s onward. In women, sarcopenia, involving simultaneous decreases in muscle strength and mass, occurs around 55 years of age, and its prevalence increases drastically from 15~25% before 70 years of age to 40% after 80 years of age (Newsmp, 2017). Based on the theoretical basis that falls among elderlies occur from loss of sense of balance due to diminished muscle functions caused by sarcopenia, most studies to date have investigated fall prevention and efforts to determine the causes of falls (Benjuya, Melze, & Kaplanski, 2004; Bergland, Jarnlo, & Laake, 2003; Buchner et al., 1997; Campbell & Robertson, 1999; Carter et al., 2001; Casteel, Peek-Asa, Lacsamana, Vazquez, & Kraus, 2004; Collins & De Luca, 1993, 1995; Ferine, Gryfe, Holiday, & Liewellyn, 1982; Hughes et al., 2001; Judge, Linsay, Underwood, & Winseminus, 1993; Laughton et al., 2003; Maki, Holliday, Topper, 1998; Mariano, 2008; Melzer & Oddsson, 2004; Melzer, Kurz, & Oddsson, 2010; Moore, Korff, & Kinzey, 2005; Owings, Pavol, Foley, & Grabiner, 2000; Park, Choi, & Hwang, 2002; Persch, Ugrinowitsch, Pereira, & Rodacki, 2009; Piirtola & Era, 2006; Rubenstein, Josephson, & Trueblood, 2000; Ryu, 2008; Schonfelder, 2000; Schoenfelder & Rubenstein, 2004; Shimada et al., 2003; Stel, Smit, Pluijm, & Lips, 2003; Yi & Ryu, 2011). However, although studies that have examined falls by determining body stability by analyzing balance have been actively pursued, many studies were conducted with an emphasis on static upright standing conditions.
Although it is difficult to analyze the actual falling motion under dynamic conditions, such as walking, in identifying its relationship to the stability of the entire body, it is possible to predict potential falls using time series data under dynamic conditions to examine local sta- bility (Dingwell, Cusumano, Sternad, & Cavanagh, 2000). Observation of stability while walking, which is one of the most common environments under which falls among elderlies often occur (Kim, 2003; Rose & Gable, 2006), is important not only for understanding the pattern of joint motion involved in postural control mechanisms but also for predicting potential falls. It is meaningful to study fall-related joint stability in the lower extremities of elderly women who have a relatively higher fall rate than elderly men, whose muscle mass decreases after menopause as their female hormone, estrogen, level decreases, and who are more vulnerable to falls from their diminished ability to maintain posture due to reduced bone density (Health Chosun, 2017; Jeon, Jeong, & Choe, 2001).
The methods for analyzing the stability of the lower extremity joints during walking include methods that presume that few steps or strides have the same periodicity in taking some portions to quantify stability¬related factors and methods that make continuous observations of steps or strides under a set time series (Verghese, Holtzer, Lipton, & Wang, 2009). Even experienced race walking athletes are known not to show the same periodicity of steps or strides during walking (Preatoni, Ferrario, Dona, Hamill, & Rodano, 2010). Changes in gait periodicity re- present outcomes from environmental changes, training, latent diseases, and unstable recovery impacting the neuromuscular tissues (Hausdorff et al., 1994; Hausdorff et al., 1997; Nakamura, Meguro, & Sasaki, 1996; Papadakis et al., 2009; Preatoni et al., 2014). Consequently, it becomes necessary to quantify gait parameters using time series data for pre- dicting potential falls through stability indices (Hahn & Chou, 2003; Hausdorff, Rios, & Edelberg, 2001; Verghese et al., 2009). Among time series analysis methods, the approximate entropy (ApEn) technique is being used as a tool to determine stability by quantifying regularity characteristics in living systems (Preatoni et al., 2014). Therefore, the ApEn technique can be used to estimate potential fall risks during walking in elderlies.
The objective of the present study was to analyze the local stability in elderly women during walking using a non-linear ApEn technique to compare the periodicity of the flexion/extension motion of their lower extremity joints on sagittal plane with that of younger women. Prior to ApEn calculation, a surrogate data test was performed to identify the dynamic neuromotor characteristics of the lower extremity flexion/ extension time series data. The differences in the periodicity of the lower extremities between the two groups, as analyzed in the present study, were assumed to be attributable to age.
1. Participants
The present study included a total of 36 participants: 18 young and 18 elderly women. The detailed physical characteristics and walking speed of these participants are shown in (Table 1).
|
Age |
Body
mass (kg) |
Height |
Walking
speed |
|
|
Young |
21.2±1.6 |
57.1±6.1 |
1.61±0.04 |
1.01±0.15 |
|
Elderly |
66.4±1.2 |
55.4±8.3 |
1.56±0.04 |
0.77±0.11 |
2. Data collection
To examine the local stability of the participants via analysis of the periodicity of flexion/extension motions of the lower extremities during walking, treadmill walking (instrumented dual belt treadmills, Bertec, USA) was used in the study. For observations on the hip, knee, and ankle movements during walking, six interconnected infrared cameras (Oqus 300, Qualisys, Switzerland) were installed near the walking space of the treadmill to capture the entire lower extremities of the participants. Next, an L-shaped frame with four markers attached and a T-shaped frame with two markers attached 75 cm apart were used to attempt spatial mapping via a nonlinear transformation (NLT) method prior to obtaining the actual coordinates. The room coordinate system was established on the right-hand side behind the treadmill where the L-shaped frame had been placed, and the axial directions were set to +Z as the vertical direction, +Y as the direction of walking, and +X as the direction to the right of the point crossing from +Y to +Z. The local coordinate axes x, y, and z for the lower extremity segments were set to the same directions as those of the room coordinate system. For the acquisition of 3-dimensional (3D) kinematic data on the hip, knee, and ankle joints, a total of 12 reflective markers were attached: three each to the sacral region, thigh, shin, and foot. The cameras were operated at 200 Hz/s by the program designated by the computer.
For the standing calibration on all participants prior to actual walking or establishing the neutral position that would serve as the reference points of the markers, images were acquired in the standing position with a sampling rate of 200 Hz for 2 sec. The participants positioned their feet to point forward at shoulder width apart, while the hip and knees were fully extended and the ankles maintained at an angle of about 90°. The data collection involved taking at least 20 strides without the participants being aware while each of them performed a full gait pattern. Walking was performed as a heel strike type of walking, a natural type of walking, which was taken into account prior to selecting the participants. The walking speed considered the speed preferred by the participants when they walk normally. Prior to data collection, all participants were given sufficient warm up time to become acclimated to walking on the treadmill.
3. Data analysis
The calculation of the 3D angles of the hip, knee, and ankle joints during walking used a joint coordinate system method (Hamill & Ryu, 2003) to calculate 20 strides, and among these, only the flexion/ extension angles with a high reliability and reproducibility, as well as a large range of motion (Preatoni et al., 2014), were selected for the examination of periodicity. The periodicity assessment used a non-linear technique of ApEn. ApEn is a method used to assess periodicity (repea- tability and continuity), which has the goal of comparing similar patches in "m" points of data and similar patches in "m+1" points. In other words, as a method that calculates "m/m+1", ApEn values go from 0 to an integer, with large values representing instability with a low perio- dicity and small values representing stability with a high periodicity. ApEn (m, r, and N) is comprised of "N" input data points u(1), u(2), ...u(N), with two input parameters "m" and "r". The input parameter "m" re- presents the pattern length being compared, while "r" is the allowable tolerance. Precedent studies were referenced for the detailed steps involved in the ApEn calculation (Stergiou, 2004; Ryu, 2016). Moreover, to test the assumption that the observed time series data represented the outcome of definitive dynamic types of the analyzed system (Theiler, Eubank, Longtin, Galdrikian, & Farmer, 1992), ApEn values were cal- culated after performing a surrogate data test (pseudo-periodic surro- gate) on the time series data on 20 strides. The calculated values were averaged and compared with the ApEn values of the original time series data (Preatoni et al., 2010).
4. Statistical analysis
Since the data analyzed in the present study cannot be assumed to show normality, the statistical significance was tested using a non-parametric method, the details of which were as follows. First, the Wilcoxon-signed rank test was performed to compare the within-group differences between the ApEn values of the lower extremity flexion/ extension angles and their surrogate ApEn values. Next, the Mann-Whitey test was performed to examine the between-group differences in the ApEn values of the flexion/extension angles for each lower extremity joint. Afterwards, the Kruskal-Wallis test was performed to examine the within-group differences in the ApEn values of the lower extremity flexion/extension angles between the joints. If the results showed a statistical difference, the Mann-Whitey test was used to determine the differences between the joints, and the statistical signifi- cance was tested via Bonferroni correction. The threshold for statistical significance was set to 0.05%.
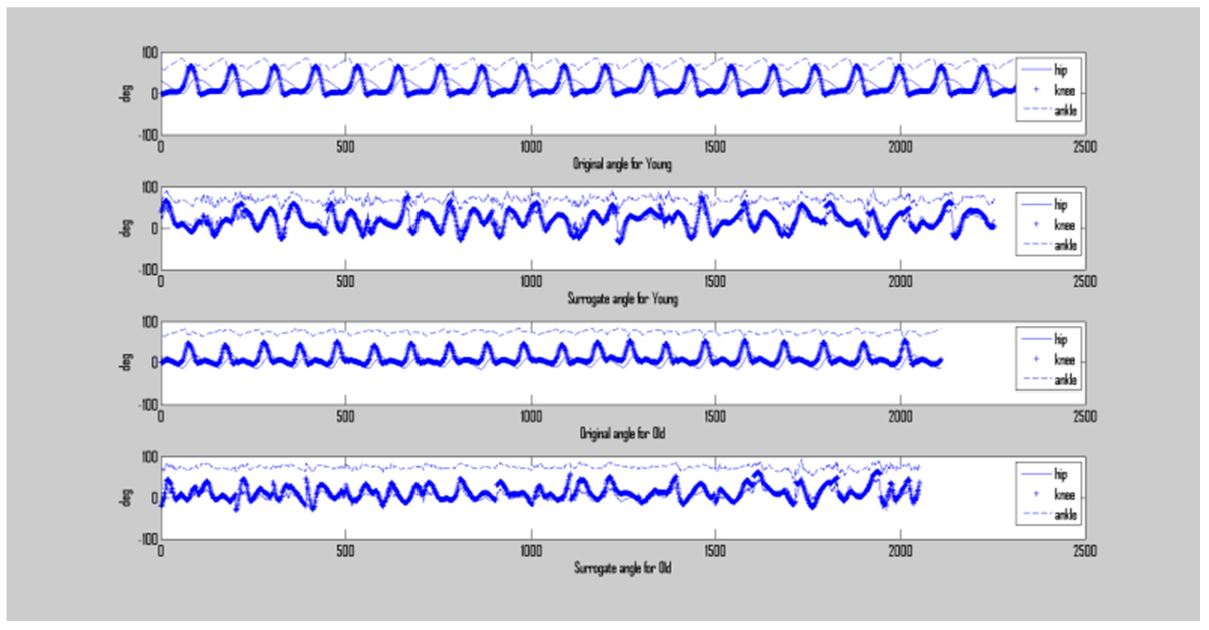
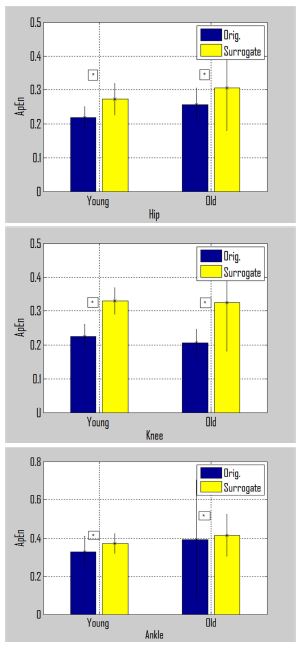
The analysis results are shown in (Figure 1, Figure 2, Figure 3, Figure 4). As shown in (Figure 2), the ApEn values after the surrogate data test showed an increased flexion/extension in the hip, knee, and ankle joints compared with the ApEn values for the time series data in both the young and elderly women groups. The ApEn values of the hip flexion/extension angle during walking in the young women group showed an average median and interquartile range of 0.218±0.032, while the ApEn values from the surrogate data test showed an average of 0.273±0.047, which represented an increase of 25% compared with the original data (p=.0001). In the elderly women group, the ApEn values of the hip flexion/extension angle showed an average median and interquartile range of 0.256±0.050, while the ApEn values from the surrogate data test showed an average of 0.306±0.126, representing a 20% increase (p=.007). Therefore, the increase in the ApEn values in the elderly women group was slightly lower than that in the young women group. With respect to the ApEn values of the knee flexion/extension angles, the young women group showed an average median and interquartile range of 0.225±0.035, while the ApEn values from the surrogate data test showed an average median and interquartile range of 0.330±0.039, representing an increase of 46% (p=.0001). In the elderly women group, the ApEn values showed an average median and interquartile range of 0.206±0.040, while the corresponding ApEn values from the surrogate data test showed an average median and interquartile range of 0.325±0.143, representing an increase of 57% (p=.0008). With respect to the ApEn values of the ankle flexion/extension motion, the young women group showed an average median and interquartile range of 0.330±0.082, while the corresponding ApEn values from the surrogate data test showed an average median and interquartile range of 0.374±0.052; this represented an increase of 12%, and the subsequent Wilcoxon-signed rank test results showed a p-value of .0053, which was lower than the significance level of 0.05 (p<.05). Meanwhile, the ApEn values of the ankle flexion/extension motion in the elderly women group showed an average median and interquartile range of 0.393±0.310, while the ApEn values from the surrogate data test showed an average median and interquartile range of 0.417±0.111; this represented an increase of 11%, and the Wilcoxon-signed rank test results showed a p-value of .00028 (p<.05).
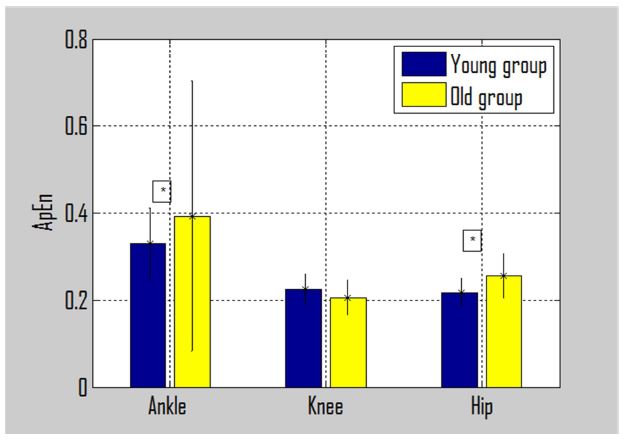
As shown in (Figure 3), the analysis of the ApEn values of the hip flexion/extension motion from the original data of the young and elderly women groups indicated that the elderly women group showed sta- tistically significantly high values, indicating a low periodicity (p=.0025). Similar results were found in the ankles as well. The Mann-Whitey test results on the differences in the ApEn values of the original data on ankle flexion/extension motion between the young and elderly women groups showed that the elderly women group had a significantly higher periodicity than the young women group (p=.026). However, there were statistically significant differences in the ApEn values of knee flexion/ extension between the young and elderly women groups (p=.763).
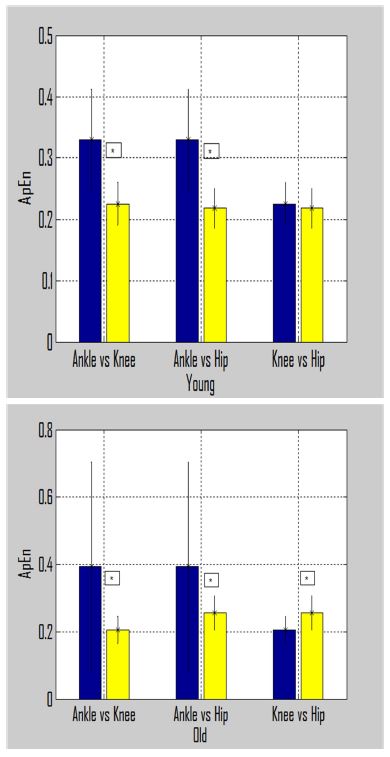
As shown in (Figure 4), the analysis results using the Kruskal-Wallis test for the significant within-group differences in the ApEn values of the joint flexion/extension angles showed that there were significant differences in the ApEn values of the hip, knee, and ankle flexion/ extension motions in both the young and elderly women groups (young women group; χ2=35.17 p=.0001; elderly women group χ2= 36.24, p=.0001). The post-hoc test results of these differences were analyzed using the Mann-Whitey test and Bonferroni correction. The results showed that there were differences in periodicity between the ankle and hip and between the ankle and knee (p=.0001) in the young women group; however, there were no differences in periodicity be- tween the knee and hip (p=.571). In the elderly women group, there were significant differences in the ApEn values between the ankle and knee (p=.0001), ankle and hip (p=.0002), and knee and hip (p=.0029), exhibiting differences in periodicity of the flexion/extension motion in each joint. In other words, periodicity appeared in the lowest to the highest order of the ankle, hip, and knee.
The objective of the present study was to observe the walking motions of young and elderly women repeatedly to compare and analyze their changes in periodicity and consequently predict the potential risk of falls. First, the present study analyzed whether the changes in perio- dicity of the lower extremity flexion/extension motion during walking in the young and elderly women were due to noise or dynamic neuro- motor characteristics. Thus, the ApEn values were calculated after per- forming the surrogate data test on the lower extremity flexion/extension motion data and compared with the original ApEn values of the lower extremity flexion/extension motion data. In the present study, both the young and elderly women groups showed a statistically significant increase in the ratios of surrogate ApEn values of the hip, knee, and ankle flexion/extension motion to those of the original data between the groups. Preatoni et al. (2010) reported an increase of 59% in the SampEn value after a surrogate data test on hip flexion/extension angle data of race walking athletes, which was higher than the results in the present study. It is believed that such a difference may be attributed to movement speed and other factors. Whatever the case may be, the ApEn values from the original time series and surrogate data tests show differences in their rate of increase; however, the increased values are consistent with the results reported by precedent studies (Bartlett, Wheat, & Robins, 2007; Riley & Turvey, 2002). Based on these results, it is believed that in both young and elderly women groups, the perio- dicity of lower extremity joint flexion/extension motion possesses not only noise during walking but also a non-linear structure, indicating a functional information on the neuroskeletal system (Preatoni et al., 2010). Therefore, it is believed that the time series data on lower extremity joint flexion/extension motion during walking may be used without any problems in determining the local postural stability.
With respect to the differences in the periodicity of lower extremity joint flexion/extension motion between the young and elderly women groups, statistically significant differences were not found in the knee, but in the hip and ankle; the elderly women group showed a signifi- cantly lower periodicity than the young women group. It is believed that this is because the elderly women have a relatively weaker hip flexor and extensor muscles than the young women, resulting in a lower periodicity of flexion/extension motion during walking and sub- sequently in a local postural instability in the hips. The neuromusculo- skeletal system is affected by various internal and external environments. Kinetic, morphological, and anatomical characteristics with environmental factors and task constraints have an impact on periodicity during body movements (Newell, Deutsch, Sosnoff, & Mayer-Kresss, 2006). Periodicity of the ankle showing a greater decrease in the elderly women group than in the young women group is believed to be attributable to elderly women having a relatively longer ankle muscle contraction and greater muscle mass loss near the ankle than young women (Kesher, Allum, & Honegger, 1993).
The results in the present study showed that the elderly women had a lower periodicity of the hip and ankle flexion/extension than the young women, which reduced their gait stability. Accordingly, it is believed that there is a high probability of potential risks of falls among elderlies being initiated from the hip and ankle joints (Holt, Jeng, Ratcliffe, & Hamill, 1995; Maik, 1997; Winter, 1983). Consequently, for elderly women to be free from falls by maintaining their dynamic sta- bility while walking, it is necessary to strengthen the muscles near the hip joint involved in hip flexion/extension motion, including the gluteus maximus, psoas major, sartorius, biceps femoris, semimembranosus, and semitendinous muscles. Moreover, the muscles near the ankle joint, such as the tibialis anterior, gastrocnemius, soleus, and plantaris muscles, should also be strengthened, while attention should also be paid to improving postural control to maintain normal proprioceptive functions (Shimada et al., 2003).
One of the points of interest in the present study was to examine the lower extremity flexion/extension during walking in the young and elderly women groups. The results showed that the young women group had the lowest ApEn value in the hip joint and the highest value in the ankle joint. Conversely, the elderly women group had the highest value in the ankle joint, as in the young women group; however, the lowest ApEn value was found in the knee joint, thereby showing a different pattern than the young women group. In other words, the young women group showed an unstable posture in going from a proximal joint to a distal joint, whereas the elderly women group showed an instability in the flexion/extension motion in the order of the ankle, hip, and knee. Therefore, it is determined that an utmost effort is needed to strengthen the hip joint muscles among all of the lower extremity joints in elderly women. The results that showed the lower periodicity of ankle flexion/extension than that of the two other joints during walking for both the young and elderly women groups may be viewed as the outcome of a relatively weaker ankle flexion/ extension capacity than that of the two other joints and relatively greater load from the ground exerted on the ankles while walking. In addition, it is speculated that such findings may be the outcome of the proximal joints acting to control the freedom of flexible body movements to adapt to unpredictable environments, such as falling, while walking (Preatoni et al., 2014).
The objective of the present study was to determine the local stability by analyzing periodicity using time series data on the lower extremity joint flexion/extension motion in the elderly during walking. Based on the findings of the present study, the following conclusions were derived:
First, it is determined that since the data of the hip and knee flexion /extension motion during walking in the young and elderly women include biological information of a kinetic system, such data can be utilized in determining local stability.
Second, with respect to the periodicity of lower extremity joint flexion /extension motion during walking, periodicity was high in the hip joint among the young women and in the knee joint among the elderly women. It is determined that because the results appeared differently, such findings can not only be used as a characteristic indicator for determining local stability during walking in the elderly but can also provide insight into predicting potential falls.
Third, the periodicity of lower extremity joint flexion/extension during walking showed opposite trends with the young women having de- creased periodicity in going from the hip to the knee joints and elderly women from the knee to the hip joints. It is determined that such findings can be used in describing walking characteristics based on age.
References
1. American geriatrics S, British Geriatrics S. (2001). American academy of orthopaedic surgeons panel on falls guideline for the prevention of falls in older person. Journal of American Geriatrics Society, 49, 664-672.
Crossref
Google Scholar
2. Bartlett, R., Wheat, J. & Robins, M. (2007). Is movement variability important for sports biomechanics? Sports Biomechanics, 6, 224-243.
Crossref
Google Scholar
3. Benjuy, N., Melze, I. & Kaplanski, J. (2004). Aging-induced shifts from a reliance on sensory input to muscle co-contraction during balanced standing. Journals of Gerontology Series A., Biological Sciences and Medical Sciences, 59(2), 166-171.
Crossref
Google Scholar
4. Bergland, A., Jarnlo, G. B. & Laake, K. (2003). Predictor of falls in the elderly by location. Aging Clinical and Experimental Research, 15, 43-50.
Crossref
Google Scholar
PubMed
5. Berry, S. D. & Miller, R. R. (2008). Falls: Epidemiology, pathophysiology, and relationship to fracture. Current Osteoporosis Reports, 6(4), 149-154.
Crossref
Google Scholar
6. Buchner, D. M., Cress, M. E., de Lateur, B. J., Esselman, P. C., Margherita, A. J., Price, R. & Wagner, E. H. (1997). The effects of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. Journal of Gerontology, 52(4), 218-224.
Crossref
Google Scholar
7. Campbell, A. J. & Robertson, M. (1999). Falls prevention over 2 years: A randomized controlled trial in woman 80 yrs and older. Age & Ageing, 28, 513-518.
Crossref
Google Scholar
8. Carter, N. D., Khan, K. M., Petit, M. A., Heinonen, A., Waterman, C., Donaldson, M. G., Janssen, P. A., Mallinson, A., Riddell, L., Kruse, K., Prior, J. C. & McKay, H. A. (2001). Results of a 10week community based strength and balance training program to reduce fall risk factors: a randomized controlled trial in 65~75 year old women with osteoporosis. British Journal of Sports Medicine, 35, 1-3.
Crossref
Google Scholar
9. Casteel, C., Peek-Asa, C., Lacsamana, C., Vazquez, L. & Kraus, J. F. (2004). Evaluation of a falls prevention program for independent elderly. American Journal of Health Behavior, 28(1), 51-60.
Crossref
Google Scholar
10. Collins, J. J. & De Luca, C. J. (1993). Open-loop and closed-loop control of posture -a random walk analysis of center of pressure tra- jectories. Experimental Brain Research, 95, 308-318.
Crossref
Google Scholar
11. Collins, J. J. & De Luca, C. J. (1995). The effects of visual input on open-loop and closed-loop postural control mechanisms. Experimental Brain Research, 103(1), 151-163.
Crossref
Google Scholar
12. Curry, L. C. & Hogstel, M. O. (2002). Nursing assessment and inter- vention: Preventing fall-related injuries in long-term care facilities. Annals of Long-term Care, 10, 29-35.
Crossref
13. Dingwell, J. B., Cusumano, J. P., Sternad, D. & Cavanagh, P. R. (2000). Slower speeds in patients with diabetic neuropath lead to improved local dynamics stability of continuous overground walking. Journal of Biomechanics, 3, 1269-1277.
Crossref
Google Scholar
14. Ferine, G. R., Gryfe, C. I., Holiday, P. J. & Liewellyn, A. (1982). The relationship of postural sway in standing to the incidence of falls in geriatric subjects. Age and Aging, 11(1), 11-16.
Crossref
Google Scholar
PubMed
15. Hahn, M. E. & Chou, L. S. (2003). Can motion of individual body segments identify dynamic instability in the elderly? Clinical Bio- mechanics, 18, 737-744.
Crossref
Google Scholar
PubMed
16. Hamill, J. & Ryu, J. (2003). Experiment in sport biomechanics. Daehan- media, 111-121.
Crossref
17. Hausdorff, J. M., Forman, D. E., Ladin, Z., Goldberger, A. L., Gigney, D. R. & Wei, J. Y. (1994). Increased walking variability in elderly persons with coggestive heart failure. Journal of American Geriatrics Society, 42, 1056-1061.
Crossref
Google Scholar
18. Hausdorff, J., Mitchell, S., Firtion, R., Peng, C., Cudkowicz, M. & Wei, J. (1997). Altered fractal dynamics of gait: reduced stride-interval cor- relations with aging and huntington's disease. Journal of Applied Physiology, 82, 262-269.
Crossref
Google Scholar
19. Hausdorff, J. M., Mitchell, S. L., Goldberger, A. L. & Wei, J. Y. (1997). Increased gait unsteadiness in community-dwelling elderly fallers. Archives Physical Medicine Rehabilitation, 78, 278-283.
Crossref
Google Scholar
20. Hausdorff, J., Rios, D. & Edelberg, H. (2001). Gait variability and fall risk in community-living older adults: a 1-year prospective study. Archives Physical Medicine Rehabilitation, 82, 1050-1056.
Crossref
Google Scholar
21. Health (2017). Chosun daily newspaper health section D1, Jan 11.
Crossref
22. Holt, K. G., Jeng, S. F., Ratcliffe, R. & Hamill, J. (1995). Energetic cost and stability during human walking at the preferred stride frequency. Journal of Motor Behavior, 27(2), 164-178.
Crossref
Google Scholar
23. Newsmp(2017). http://www.newsmp.com/news/articleview.html?idxno =164205
Crossref
24. Hughes, V. A., Frontera, W. R., Wood, M., Evans, W. J., Dakkak, G. E., Roubenoff, R. & Fiatarone Singh, M. A. (2001). Longitudinal muscle strength changes in older adults: influence of muscle mass, physical activity and health. Journals of Gerontology Series A., Biological Sciences and Medical Sciences, 56, B209-B217.
Crossref
Google Scholar
25. Jeon, M. Y., Jeong, H. C. & Choe, M. A. (2001). A study on the elderly patients hospitalized by the fracture from the fall. Korean Academy of Nursing, 31(3), 443-453.
Crossref
Google Scholar
26. Johnell, O. & Kanis, J. A. (2006). An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporosis International, 17, 1726-1733.
Crossref
Google Scholar
27. Judge, J. O., Linsay, C., Underwood, M. & Winseminus, D. (1993). Balance improvements in older woman: Effects of exercise training. Physical Therapy, 73(4), 254-265.
Crossref
Google Scholar
PubMed
28. Kauffman, T. L. (1999). Geriatric rehabilitation Manual. Philadelphia, Churchill Livingstone.
Crossref
Google Scholar
29. Kesher, E. A. Allum, A. H. & Honegger, F. (1993). Predictors of Less Stable Postural Responses to Support Surface Rotations in Healthy Human Elderly. Journal of Vestibular Research, 3, pp.419-429.
Google Scholar
30. Kim, C. K. (2003). An analysis of fall incidence rate and the related factors of fall in hospitalized patients, Seoul National University, Graduate School, Nursing, Thesis.
31. Laughton, C. A., Slavin, M., Katdare, K., Nolan, L., Bean, J. F., Kerrigan, D. C., Phillips, E., Lipsitz, L. A. & Collins, J. J. (2003). Aging, muscle activity, and balance control: physiologic changes associated with balance impairment. Gait & Posture, 18(2), 101-108.
Crossref
Google Scholar
32. Lord, S. R., Caplan, G. A. & Ward, J. A. (1993). Balance, reaction time, and muscle strength in exercising and non-exercising older woman: A pilot study. Archives of Physical Medicine and Rehabilitations, 74(8), 837-839.
Crossref
33. Maki, B. E. (1997). Gait changes in older adults: predictors of falls or indicators of fear? Journal of the American Geriatric Society, 45, 313-320.
Crossref
Google Scholar
PubMed
34. Melzer, I. & Oddsson, L. I. (2004). The effect of a cognitive task on voluntary step execution in healthy elderly and young individuals. Journal of the American Geriatric Society, 52(8), 1255-1262.
Google Scholar
PubMed
35. Maki, B. E., Holliday, P. J. & Topper, A. K. (1998). A prospective study of postural balance and risk of falling in an ambulatory and inde- pendent dlderly population. Journal of Gerontology, 49, 72-84.
Google Scholar
PubMed
36. Mariano, C. (2008). A 16-week tai chi program prevented falls in healthy older adults. Evidence Based Nursing, 11(2), 60.
Crossref
Google Scholar
PubMed
37. Melzer, I., Kurz, I. & Oddsson, L. I. E. (2010) A retrospective analysis of balance control parameters in elderly fallers and non-fallers. Clinical Biomechanics, 25, 984-988.
Google Scholar
38. Moore, J. B., Korff, T. & Kinzey, S. J. (2005). Acute effects of a single bout of resistance exercise on postural control in elderly persons. Perceptual and Motor Skills, 100, 725-733.
Crossref
Google Scholar
39. Nakamura, T., Meguro, K. & Sasaki, H. (1996). Relationship between falls and stride length variability in senile dementia of the Alzheimer type. Journal of Gerontology, 42, 108-113.
Crossref
Google Scholar
40. Newell, K. M., Deutsch, K. M., Sosnoff, J. J. & Mayer-Kresss, G. (2006). Variability in motor output as noise: A default and erroneous pro- position?, Movement system variability (pp.3-23). Champaign, IL: Human Kinetics.
Crossref
41. O'Brien, K. Culbam, E. & Pickles, B. (1997). Balance and Skeletal Align- ment in a Group of Elderly Female Fallers and Non-fallers. Journal of Gerontology, 52, pp.221-226.
Crossref
Google Scholar
PubMed
42. Owings, T. M., Pavol, M. J., Foley, K. T. & Grabiner, M. D. (2000). Measures of postural stability are not predictors of recovery from large postual disturbances in healthy older adults. Journal of the American Geriatric Society, 48, 42-50.
Google Scholar
43. Papadakis, N. C., Christstakis, D. G., Tzagarakis, G. N., Chlouverakis, G. I., Kampanis, N. A. & Stergiopoulos, K. N. (2009). Gait variability mea- suremrnts in lumbar spinal stenosis patients. Physiological Mea- surement, 1171.
Crossref
Google Scholar
44. Park, J. S., Choi, E. Y. & Hwang, T. Y. (2002). The effects of streng- thening leg muscular strength on the elderly's walking and balance ability. Journal of Korean Society of Physical Therapy, 14(2), 71-79.
45. Persch, L. N., Ugrinowitsch, C., Pereira, G. & Rodacki, A. L. F. (2009). Strength training improves fall-related gait kinematics in the elderly: A randomized controlled trial. Clinical Biomechanics, 24, 819-825.
Crossref
Google Scholar
46. Piirtola, M. & Era, P. (2006). Force platform measurements as predictors of falls among older people. A Review. Gerontology, 52(1), 1-16.
Google Scholar
PubMed
47. Preatoni, E., Ferrario, M., Dona, G., Hamill, J. & Rodano, R. (2010). Motor variability in sports: A non-linear analysis of race walking. Journal of Sports Science, 28(12), 1327-1336.
Crossref
Google Scholar
PubMed
48. Preatoni, E., Hamill, J., Harrison, A. J., Hayes, K., Emmerik, V. R., Wilson, C. & Rodano, R. (2014). Movement variability and skills monitoring in sports. Sports Biomechanics, 12(2), 69-92.
Crossref
Google Scholar
PubMed
49. Riley, M. A. & Turvey, M. T. (2002). Variability of determinism in motor behavior. Journal of Motor Behavior, 34, 99-125.
Crossref
Google Scholar
PubMed
50. Rose, J. & Gable, J. G. (2006). Human walking. Williams & Wilkins, Baltimore.
Crossref
51. Ryu, J. S. (2008). Dynamic stability analysis of patients with degenerative osteoarthritis during walking. Korean Journal of Sport Biomechanics, 18(1), 12-30.
Crossref
52. Ryu, J. S. (2016). Effects of Prolonged Running-Induced Fatigue on Periodicity of Shank-Foot Segment Coupling and Free Torque. Korean Journal of Sport Biomechanics, 26(3), 257-264.
Crossref
Google Scholar
53. Rubenstein, L., Josephson, K. & Trueblood, P. (2000). Effects of a group exercise program on strength, mobility, and falls among fall-prone elderly men. Journal of Gerontology: Medical Science, 55(6), M317 -M321.
Crossref
Google Scholar
54. Schonfelder, D. P. (2000). A fall prevention program for elderly individual: exercise in long term case setting. Journal of Gerontological Nursing, 126(3), 43-51.
Crossref
PubMed
55. Schoenfelder, D. P. & Rubenstein, L. M. (2004). An exercise program to improve fall-related outcomes in elderly nursing home residents. Applied Nursing Research, 17(1), 21-31.
Crossref
Google Scholar
PubMed
56. Shimada, H., Obuchi, S., Kamide, N., Shiba, Y., Okamoto, M. & Kakurai, S. (2003). Relationship with dynamic balance function during standing and walking. American Journal of Physical and Medicine Rehabili- tation, 83(7), 511-516.
Crossref
Google Scholar
57. Song, K. A., Mun, J. S., Kang, S. S. & Choi, J. H. (2001). The Survey of Activities and Fear of Falling in the Community Dwelling Elderly. Journal of Korean Public Health Nursing, 15(2), 324-333.
Crossref
Google Scholar
58. Statics Korea, Korean statical information service; http://www.kosis.kr, 2014, 2016.
Crossref
59. Stel, V. S., Smit, J. H., Pluijm, S. M. & Lips, P. (2003). Balance and mobility performance as treatable risk factors for recurrent falling in older persons. Journal of Clinical Epidemiology, 56, 659-668.
Crossref
Google Scholar
60. Stergiou, N. (2004). Innovative analyses of human movement-analytical tools for human movement. Human Kinetics.
Crossref
61. Theiler, J., Eubank, S., Longtin, A., Galdrikian, B. & Farmer, D. (1992). Testing for nonlinearity in time series: the method of surrogate data. Physica D58, 77-94.
Crossref
Google Scholar
62. Tinetti, M. E., Speechley, M. & Ginter, S. F. (1988). Risk factors for falls among elderly persons living in the community. New England Journal of Medicine, 319, 1701-1707.
Crossref
Google Scholar
PubMed
63. Verghese, J., Holtzer, R., Lipton, R. B. & Wang, C. (2009). Quantitative gait markers and incident fall risk in older adults. Journals of Gerontology Series A., Biological Sciences and Medical Sciences, 64A, 896-901.
Google Scholar
64. Winter, D. A. (1983). Biomechanical motor patterns in normal walking. Journal of Motor Behavior, 15(4), 302-330.
Crossref
Google Scholar
65. Wolfson, L., Judge, J. & Whipple, R. (1995). Strengthening is a Major Factor in Balance, Gait and the Occurrence of Falls. Journal of Gerontology, 50, pp.64-67.
Crossref
Google Scholar
PubMed
66. Yi, J. H. & Ryu, J. S. (2011). Biomechanical alternation of the elderly depending on the type of gait termination. Korean Journal of Sport Biomechanics, 21(2), 189-196.
Crossref
Google Scholar
